A new University of Minnesota study reveals that treated municipal wastewater -- even wastewater treated by the highest-quality treatment technology -- can result in significant quantities of antibiotic-resistant bacteria, often referred to as "superbacteria," in surface waters. The study also suggests that standard wastewater treatment technologies probably release far greater quantities of antibiotic-resistant genes used by bacteria, but this likely goes unnoticed because background levels of bacteria are normally much higher than in the water studied in this research.
The new study is led by civil engineering associate professor Timothy LaPara in the University of Minnesota, Twin Cities College of Science and Engineering. The study is published in the most recent issue of Environmental Science and Technology, a journal of the American Chemical Society. The research was part of a unique class project in a graduate-level civil engineering class at the University of Minnesota focused on environmental microbiology.
Antibiotics are used to treat numerous bacterial infections, but the ever-increasing presence of antibiotic-resistant bacteria has raised substantial concern about the future effectiveness of antibiotics. In response, there has been increasing focus on environmental reservoirs of antibiotic resistance over the past several years. Antibiotic use in agriculture has been heavily scrutinized, while the role of treated municipal wastewater has received little attention as a reservoir of resistance.
Antibiotic-resistant bacteria develop in the gastrointestinal tracts of people taking antibiotics. These bacteria are then shed during defecation, which is collected by the existing sewer infrastructure and passed through a municipal wastewater treatment facility.
In this study, the Ph.D. students and professor examined the impact of municipal wastewater in Duluth, Minn., on pristine surface waters by gathering water samples from the St. Louis River, Duluth-Superior Harbor, and Lake Superior in northeastern Minnesota. The treatment facility in Duluth is considered one of the best. After solids and biological matter are removed, the Duluth wastewater treatment is one of only a few in the country that filter water a third time through a mixed media filter to remove additional particles of bacteria and nutrients. Standard wastewater treatment treats water twice to remove solids and biological matter.
"This was a unique and ideal location for this study because of the exemplary wastewater treatment mixed with surprisingly pristine surface waters with very low background levels of bacteria that wouldn't mask our results," LaPara said. "Previous studies in which treated municipal wastewater was implicated as a source of antibiotic resistance were more convoluted because multiple sources of antibiotic resistance genes existed, such as agricultural activity and industrial wastewater discharges."
While the levels of overall bacteria were still relatively low in the surface water samples, researchers in the University of Minnesota study found that the quantities of antibiotic-resistant genes and human-specific bacteria were typically 20-fold higher at the site where treated wastewater was released into the Duluth-Superior Harbor compared to nearby surface water samples.
"Current wastewater treatment removes a very large fraction of the antibiotic resistance genes," LaPara said. "But this study shows that wastewater treatment operations need to be carefully considered and more fully studied as an important factor in the global ecology of antibiotic resistance."
In addition to LaPara, researchers involved in the study include civil engineering Ph.D. students Tucker Burch, Patrick McNamara, David Tan; and bioproducts and biosystems engineering Ph.D. student Mi Yan, with help from soil, water and climate Ph.D. student Jessica Eichmiller.
The University of Minnesota research study was funded by the National Science Foundation's broader impacts effort, which combines research and education. The Minnesota Environment and Natural Resources Trust Fund paid for time on the R/V Blue Heron ship to collect water samples.
**Source: University of Minnesota
15 November 2011
El 30% de los hombres que consume más de 10 fármacos sufre disfunción eréctil
Cuantos más fármacos consuma un hombre, mayor será su riesgo de padecer disfunción eréctil. Acudir a la consulta del médico para revisar su medicación puede mejorar el problema, ya que es posible que tome medicamentos que ya no le hacen falta, que estén duplicados o que aporten más efectos secundarios que beneficios.
La edad, la obesidad, el tabaco, las enfermedades cardiovasculares y la diabetes son algunos de los principales factores que aumentan el riesgo de impotencia. Según un estudio que recoge la última edición de la revista 'British Journal of Urology International', a esta lista hay que añadir el consumo de múltiples fármacos.
Un equipo de investigadores del Centro Médico Kaiser Permanente de Los Ángeles (Estados Unidos) ha analizado los datos de más de 37.000 hombres de entre 45 y 69 años y ha comprobado que el 16% de los que toman hasta dos fármacos al día sufre disfunción eréctil moderada, porcentaje que asciende a casi el 20% de quienes consumen de tres a cinco medicamentos, al 25% de los que ingieren entre seis y nueve y, por último, se acerca al 31% de aquellos que toman más de 10 productos cada día.
Los autores del estudio señalan que los fármacos más asociados a la impotencia son los antihipertensivos y determinados productos destinados a tratar problemas mentales como la depresión. Asimismo, la potencia sexual se ve mermada con todos los fármacos que interfieren en la función de la hormona testosterona.
Además de revisar la medicación para evaluar qué fármacos son prescindibles, los autores del estudio proponen el fomento de "cambios en el estilo de vida, como modificar la dieta, hacer ejercicio regular y no fumar, lo que puede ayudar a controlar la hipertensión, la diabetes y el estrés y reducir el riesgo de disfunción eréctil. Los médicos pueden aprovechar para hablar con sus pacientes sobre los riesgos asociados a la impotencia y los problemas de salud que hacen necesario consumir múltiples fármacos".
El especialista español Ignacio Moncada, coordinador del Grupo de Andrología de la Asociación Española de Urología, confirma que el fomento de hábitos saludables es el primer paso para combatir el problema. "Si a pesar de eso no mejora la función sexual, habrá que ver qué tratamiento se aplica".
Asimismo, Moncada cree necesario un uso racional de los medicamentos en personas con enfermedades crónicas. Una evaluación cuidadosa puede reducir significativamente el número de productos que consume una persona. "Hay medicaciones que se ponen pero luego nadie las quita cuando ya no son indispensables", reconoce.
"A veces me llegan pacientes que podrían tratarse con fármacos específicos para la impotencia, pero existe una incompatibilidad con los parches de nitroglicerina que están usando", comenta el urólogo. "La mayoría de las veces se los pusieron después de una angina de pecho, pero ya no son necesarios. Les digo que pregunten a su cardiólogo y la mayoría de las veces éste les confirma que pueden dejar de utilizarlos".
No obstante, no siempre se pueden dejar de tomar los medicamentos prescritos. Al fin y al cabo, los hombres con impotencia suelen ser aquellos con una salud más precaria, que son precisamente los que necesitan más medicación. "A veces no es posible saber si lo que causa la disfunción eréctil es el fármaco o la enfermedad", asegura Moncada. Así, los productos para la hipertensión causan impotencia, pero esta patología también es, por sí sola, una de las principales causas del problema sexual.
**Publicado en "EL MUNDO"
La edad, la obesidad, el tabaco, las enfermedades cardiovasculares y la diabetes son algunos de los principales factores que aumentan el riesgo de impotencia. Según un estudio que recoge la última edición de la revista 'British Journal of Urology International', a esta lista hay que añadir el consumo de múltiples fármacos.
Un equipo de investigadores del Centro Médico Kaiser Permanente de Los Ángeles (Estados Unidos) ha analizado los datos de más de 37.000 hombres de entre 45 y 69 años y ha comprobado que el 16% de los que toman hasta dos fármacos al día sufre disfunción eréctil moderada, porcentaje que asciende a casi el 20% de quienes consumen de tres a cinco medicamentos, al 25% de los que ingieren entre seis y nueve y, por último, se acerca al 31% de aquellos que toman más de 10 productos cada día.
Los autores del estudio señalan que los fármacos más asociados a la impotencia son los antihipertensivos y determinados productos destinados a tratar problemas mentales como la depresión. Asimismo, la potencia sexual se ve mermada con todos los fármacos que interfieren en la función de la hormona testosterona.
Además de revisar la medicación para evaluar qué fármacos son prescindibles, los autores del estudio proponen el fomento de "cambios en el estilo de vida, como modificar la dieta, hacer ejercicio regular y no fumar, lo que puede ayudar a controlar la hipertensión, la diabetes y el estrés y reducir el riesgo de disfunción eréctil. Los médicos pueden aprovechar para hablar con sus pacientes sobre los riesgos asociados a la impotencia y los problemas de salud que hacen necesario consumir múltiples fármacos".
El especialista español Ignacio Moncada, coordinador del Grupo de Andrología de la Asociación Española de Urología, confirma que el fomento de hábitos saludables es el primer paso para combatir el problema. "Si a pesar de eso no mejora la función sexual, habrá que ver qué tratamiento se aplica".
Asimismo, Moncada cree necesario un uso racional de los medicamentos en personas con enfermedades crónicas. Una evaluación cuidadosa puede reducir significativamente el número de productos que consume una persona. "Hay medicaciones que se ponen pero luego nadie las quita cuando ya no son indispensables", reconoce.
"A veces me llegan pacientes que podrían tratarse con fármacos específicos para la impotencia, pero existe una incompatibilidad con los parches de nitroglicerina que están usando", comenta el urólogo. "La mayoría de las veces se los pusieron después de una angina de pecho, pero ya no son necesarios. Les digo que pregunten a su cardiólogo y la mayoría de las veces éste les confirma que pueden dejar de utilizarlos".
No obstante, no siempre se pueden dejar de tomar los medicamentos prescritos. Al fin y al cabo, los hombres con impotencia suelen ser aquellos con una salud más precaria, que son precisamente los que necesitan más medicación. "A veces no es posible saber si lo que causa la disfunción eréctil es el fármaco o la enfermedad", asegura Moncada. Así, los productos para la hipertensión causan impotencia, pero esta patología también es, por sí sola, una de las principales causas del problema sexual.
**Publicado en "EL MUNDO"
AMD-like lesions delayed in mice fed lower glycemic index diet
Feeding older mice a lower glycemic index (GI) diet consisting of slowly-digested carbohydrates delays the onset of age-related, sight-threatening retinal lesions, according to a new study from the Laboratory for Nutrition and Vision Research at the Jean Mayer USDA Human Nutrition Research Center on Aging (USDA HNRCA) at Tufts University. The researchers studied middle-aged and older mice that consumed either a higher or lower GI diet. Mice fed the lower GI diet developed fewer and less-severe age-related lesions in the retina than the mice fed the higher GI diet. The lesions included basal laminar deposits, which typically develop after age 60 in the human retina and are the earliest warning sign of Age-Related Macular Degeneration (AMD).
"To our knowledge, we have established the first mature, mammalian model indicating a delay in the development of AMD-like lesions as the result of a lower GI diet," says Allen Taylor, PhD, director of the Laboratory for Nutrition and Vision Research at the USDA HNRCA. "The only difference between the two groups of mice we studied is the GI of their meals, which suggests that diet alone is enough to accelerate or delay the formation of lesions. These results, coupled with similar observations made by our laboratory in earlier human epidemiologic studies imply that lower GI diets hold potential as an early intervention for preventing onset and progress of AMD."
The dietary glycemic index (DGI) measures the rate at which glucose is delivered to the bloodstream after consuming carbohydrates. Higher GI foods including white bread and white potatoes trigger a rapid delivery of glucose that pushes the body to work overtime to absorb, whereas lower GI foods, like whole grain bread and fruits and vegetables, initiate a slower release of glucose that is more easily processed by cells.
Compared to the mice on the lower GI diet, mice on the higher GI diet demonstrated elevated accumulations of debris known as advanced glycation end products (AGEs) in the whole retina, particularly in the cells of the RPE. The RPE plays a crucial role in maintaining vision and its dysfunction results in the gradual central vision loss that is the hallmark of AMD. AGE accumulation has also been linked to tissue damage in other age-related diseases such as Type 2 diabetes and cardiovascular disease.
"We presume the elevated accumulation of AGEs we saw in the retina of the higher GI group is associated with toxicity. The AGEs result from the modification of proteins by excess glucose and this compounds the normal protein damage that happens as we age," says Karen Weikel, first author and a PhD candidate at the Friedman School of Nutrition Science and Policy at Tufts. "While previous research has linked higher GI diets to AGE accumulation in the blood, ours appears to be the first to show diet-related AGE presence in tissue, such as the retina, which becomes the site of the eye disease."
The research, published online in October in the journal Aging Cell traces the drop-off in AGE accumulation in the lower GI diet to the ubiquitin-protease system pathway and the lysosome/autophagy pathway. "In cell models we saw that both the ubiquitin pathways and lysosome pathways processed proteins more efficiently and kept cells healthier when glucose levels were lower," says Taylor, who is also a professor at the Friedman School and Tufts University School of Medicine (TUSM). "Both pathways are well-known for their ability to remove damage from cells, but this had not been previously systematically explored for removal of AGEs."
The Centers for Disease Control reports AMD is the chief cause of irreparable vision loss in Americans over age 65 and that 1.8 million people in the U.S. are living with the disease, a number that is expected to approach 3 million by 2020.
"Although our laboratory has shown in epidemiological studies and now in a live laboratory model that lower GI diets may prevent or delay the progression of AMD, future studies are needed. Trials involving more animals and human clinical trials could more carefully describe the protein-editing machinery that appeared to determine the development and severity of the lesions we saw," Taylor says. "With such information, we may begin to develop cost-effective dietary interventions as well as a new generation of drugs that mimic the presumed effects of the lower GI diet to prolong vision."
The authors received funding for this study from the USDA, Johnson & Johnson Focused Giving and the National Institutes of Health (NIH).
*Source: Tufts University, Health Sciences Campus
"To our knowledge, we have established the first mature, mammalian model indicating a delay in the development of AMD-like lesions as the result of a lower GI diet," says Allen Taylor, PhD, director of the Laboratory for Nutrition and Vision Research at the USDA HNRCA. "The only difference between the two groups of mice we studied is the GI of their meals, which suggests that diet alone is enough to accelerate or delay the formation of lesions. These results, coupled with similar observations made by our laboratory in earlier human epidemiologic studies imply that lower GI diets hold potential as an early intervention for preventing onset and progress of AMD."
The dietary glycemic index (DGI) measures the rate at which glucose is delivered to the bloodstream after consuming carbohydrates. Higher GI foods including white bread and white potatoes trigger a rapid delivery of glucose that pushes the body to work overtime to absorb, whereas lower GI foods, like whole grain bread and fruits and vegetables, initiate a slower release of glucose that is more easily processed by cells.
Compared to the mice on the lower GI diet, mice on the higher GI diet demonstrated elevated accumulations of debris known as advanced glycation end products (AGEs) in the whole retina, particularly in the cells of the RPE. The RPE plays a crucial role in maintaining vision and its dysfunction results in the gradual central vision loss that is the hallmark of AMD. AGE accumulation has also been linked to tissue damage in other age-related diseases such as Type 2 diabetes and cardiovascular disease.
"We presume the elevated accumulation of AGEs we saw in the retina of the higher GI group is associated with toxicity. The AGEs result from the modification of proteins by excess glucose and this compounds the normal protein damage that happens as we age," says Karen Weikel, first author and a PhD candidate at the Friedman School of Nutrition Science and Policy at Tufts. "While previous research has linked higher GI diets to AGE accumulation in the blood, ours appears to be the first to show diet-related AGE presence in tissue, such as the retina, which becomes the site of the eye disease."
The research, published online in October in the journal Aging Cell traces the drop-off in AGE accumulation in the lower GI diet to the ubiquitin-protease system pathway and the lysosome/autophagy pathway. "In cell models we saw that both the ubiquitin pathways and lysosome pathways processed proteins more efficiently and kept cells healthier when glucose levels were lower," says Taylor, who is also a professor at the Friedman School and Tufts University School of Medicine (TUSM). "Both pathways are well-known for their ability to remove damage from cells, but this had not been previously systematically explored for removal of AGEs."
The Centers for Disease Control reports AMD is the chief cause of irreparable vision loss in Americans over age 65 and that 1.8 million people in the U.S. are living with the disease, a number that is expected to approach 3 million by 2020.
"Although our laboratory has shown in epidemiological studies and now in a live laboratory model that lower GI diets may prevent or delay the progression of AMD, future studies are needed. Trials involving more animals and human clinical trials could more carefully describe the protein-editing machinery that appeared to determine the development and severity of the lesions we saw," Taylor says. "With such information, we may begin to develop cost-effective dietary interventions as well as a new generation of drugs that mimic the presumed effects of the lower GI diet to prolong vision."
The authors received funding for this study from the USDA, Johnson & Johnson Focused Giving and the National Institutes of Health (NIH).
*Source: Tufts University, Health Sciences Campus
Stem cell study helps clarify the best time for therapy to aid heart attack survivors
A research network led by a Mayo Clinic physician found that stem cells obtained from bone marrow delivered two to three weeks after a person has a heart attack did not improve heart function. This is the first study to systematically examine the timing and method of stem cell delivery and provides vital information for the field of cell therapy. The results were presented this morning at the 2011 Scientific Sessions of the American Heart Association Meeting in Orlando, Fla.
They also will be published online in JAMA to coincide with the presentation.
"Some data suggests that stem cell therapy is helpful within the first week after a heart attack," says Robert Simari, M.D., cardiologist at Mayo Clinic and chairman of the Cardiovascular Cell Therapy Research Network (CCTRN). The network includes five clinics and other sites supported by the National Heart, Lung, and Blood Institute, part of the National Institutes of Health. "Our study helps identify the limits of when stem cell therapy might be beneficial. We now know that this therapy should not be extended two to three weeks after a heart attack. While it is safe to do so, we did not find any benefit to heart function after six months."
Between July 2008 and February 2011, 87 people with heart attacks and moderate to severe left ventricular dysfunction received their own bone marrow mononuclear stem cells (BMCs) or placebo. The study, called LateTIME, developed a standardized method of processing the BMCs and was the first such trial to provide a uniform dose to each participant.
The researchers assessed heart function through a cardiac MRI by measuring the ejection fraction, or what percentage of blood is pumped out of the left ventricle during each contraction. No significant differences were found in the cardiac function readings between baseline and six months in the BMC group (from 48.7 percent to 49.2 percent) or the placebo group (from 45.3 percent to 48.8 percent).
Dr. Simari says that earlier studies suggest patients with severe heart attacks benefit most from stem cell therapy. The researchers were interested in studying the two- to three-week period because many people who have severe heart attacks are not well enough or stable enough to receive cells right after their heart attacks. "Many are on life support or other systems, and we didn't think that studying them that early was the best way to assess the benefits to the sickest patients," Dr. Simari says.
The LateTIME study offers a cautionary lesson for people who have had heart attacks and are considering going overseas to seek stem cell treatment. "We would suggest that individuals not seek treatment outside of the U.S. for therapies that aren't proven effective," Dr. Simari says. The researchers think that the heart may be less receptive to such therapies two to three weeks after a heart attack, or that a person's stem cells are less potent at that time.
Jay Traverse, M.D., lead author of the study and a cardiologist at the Minneapolis Heart Institute at Abbott Northwestern Hospital, says patients will be followed clinically for two years in the LateTIME study.
"There may still be other benefits to stem cell therapy that may be uncovered over time," Dr. Traverse says. "We observed that patients who received the cell therapy had fewer adverse events such as placement of defibrillators or repeat revascularization compared to patients who got the placebo, consistent with observations in some of the European trials. This therapy may provide hidden safety measures that reduce adverse events and that's something we will follow closely."
LateTIME is one of three heart stem cell trials being conducted by CCTRN. The other trials will explore the effectiveness of stem cell therapy delivered at three days and seven days following a heart attack, and the usefulness of stem cell therapy in people with chronic heart failure.
*Source: Mayo Clinic
They also will be published online in JAMA to coincide with the presentation.
"Some data suggests that stem cell therapy is helpful within the first week after a heart attack," says Robert Simari, M.D., cardiologist at Mayo Clinic and chairman of the Cardiovascular Cell Therapy Research Network (CCTRN). The network includes five clinics and other sites supported by the National Heart, Lung, and Blood Institute, part of the National Institutes of Health. "Our study helps identify the limits of when stem cell therapy might be beneficial. We now know that this therapy should not be extended two to three weeks after a heart attack. While it is safe to do so, we did not find any benefit to heart function after six months."
Between July 2008 and February 2011, 87 people with heart attacks and moderate to severe left ventricular dysfunction received their own bone marrow mononuclear stem cells (BMCs) or placebo. The study, called LateTIME, developed a standardized method of processing the BMCs and was the first such trial to provide a uniform dose to each participant.
The researchers assessed heart function through a cardiac MRI by measuring the ejection fraction, or what percentage of blood is pumped out of the left ventricle during each contraction. No significant differences were found in the cardiac function readings between baseline and six months in the BMC group (from 48.7 percent to 49.2 percent) or the placebo group (from 45.3 percent to 48.8 percent).
Dr. Simari says that earlier studies suggest patients with severe heart attacks benefit most from stem cell therapy. The researchers were interested in studying the two- to three-week period because many people who have severe heart attacks are not well enough or stable enough to receive cells right after their heart attacks. "Many are on life support or other systems, and we didn't think that studying them that early was the best way to assess the benefits to the sickest patients," Dr. Simari says.
The LateTIME study offers a cautionary lesson for people who have had heart attacks and are considering going overseas to seek stem cell treatment. "We would suggest that individuals not seek treatment outside of the U.S. for therapies that aren't proven effective," Dr. Simari says. The researchers think that the heart may be less receptive to such therapies two to three weeks after a heart attack, or that a person's stem cells are less potent at that time.
Jay Traverse, M.D., lead author of the study and a cardiologist at the Minneapolis Heart Institute at Abbott Northwestern Hospital, says patients will be followed clinically for two years in the LateTIME study.
"There may still be other benefits to stem cell therapy that may be uncovered over time," Dr. Traverse says. "We observed that patients who received the cell therapy had fewer adverse events such as placement of defibrillators or repeat revascularization compared to patients who got the placebo, consistent with observations in some of the European trials. This therapy may provide hidden safety measures that reduce adverse events and that's something we will follow closely."
LateTIME is one of three heart stem cell trials being conducted by CCTRN. The other trials will explore the effectiveness of stem cell therapy delivered at three days and seven days following a heart attack, and the usefulness of stem cell therapy in people with chronic heart failure.
*Source: Mayo Clinic
Una inyección que baja el colesterol
Los pacientes incapaces de controlar con pastillas sus niveles de colesterol «malo» pueden conseguirlo con un nuevo anticuerpo inyectado, según una investigación presentada en una sesión científica de la Asociación Norteamericana del Corazón.
Las primeras pruebas en seres humanos han puesto de manifiesto que ese pinchazo bajó las lipoproteínas (colesterol «malo») en un 64%, a pacientes sanos, en comparación con los que recibieron un placebo. La sustancia inyectada es un anticuerpo monoclonal, es decir, una proteína humana hecha en laboratorio. Los anticuerpos monoclonales se usan ya para combatir determinados cánceres y otras enfermedades.
Los científicos de este estudio utilizaron el anticuerpo AMG145, que combate el regulador PCSK9 del colesterol. Este regulador es el que impide al hígado la eliminación del torrente sanguíneo del colesterol «malo».
Las primeras pruebas en seres humanos han puesto de manifiesto que ese pinchazo bajó las lipoproteínas (colesterol «malo») en un 64%, a pacientes sanos, en comparación con los que recibieron un placebo. La sustancia inyectada es un anticuerpo monoclonal, es decir, una proteína humana hecha en laboratorio. Los anticuerpos monoclonales se usan ya para combatir determinados cánceres y otras enfermedades.
Los científicos de este estudio utilizaron el anticuerpo AMG145, que combate el regulador PCSK9 del colesterol. Este regulador es el que impide al hígado la eliminación del torrente sanguíneo del colesterol «malo».
Médicos de EE.UU. muestran la mejoría de 16 pacientes infartados con sus propias células
Si el cerebro es un órgano plástico capaz de producir nuevas neuronas, ¿por qué no podría serlo también el corazón? El investigador italiano Piero Anversa persiguió esta hipótesis hasta demostrar que nuestra bomba cardiaca era capaz de regenerarse ella sola, incluso a edades avanzadas. Eso significaba que no estaba dicho todo después de un infarto y que las zonas muertas del corazón podrían volver a la vida. Solo se necesitaría un pequeño empujón desde el exterior para animar a las células madre del corazón a hacer su trabajo.
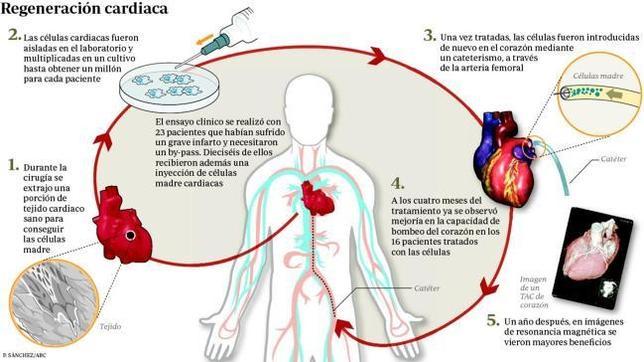
Ahora en una nueva investigación, el equipo de Anversa de la Universidad de Harvard, en colaboración con la Universidad de Louisville (Estados Unidos), muestra cómo un corazón enfermo puede repararse a sí mismo. Los investigadores trataron a 16 pacientes que habían sufrido un infarto muy severo y lograron que su corazón se recuperara tras infundirle sus propias células madre cardiacas. Los resultados se publican en la revista médica «The Lancet» y «abren una nueva opción para los pacientes infartados con un mal pronóstico», asegura Anversa .
Un año después del tratamiento, el efecto continuaba. Es la primera vez que se demuestra el efecto de una terapia celular a tan largo plazo. Eso sí, con una ayuda técnica bastante potente, no solo con un «empujoncito» exterior. Para conseguirlo, los enfermos tuvieron que pasar primero por una biopsia de corazón y después por un cateterismo, una técnica no exenta de riesgo. En la biopsia se toma parte del tejido del corazón para después aislar y ampliar en el laboratorio las células madre reparadoras. Con el cateterismo posterior, se introduce un catéter por la arteria para llegar hasta el corazón y depositar las células.
Al producirse un ataque cardiaco, el infarto reduce la capacidad que tienen los ventrículos para bombear la sangre en un solo latido. Al disminuir el aporte sanguíneo, el tejido cardiaco se queda sin oxígeno y muere. Esas zonas necrosadas provocan un falllo cardiaco, porque la capacidad de bombeo se reduce.
Ahora en una nueva investigación, el equipo de Anversa de la Universidad de Harvard, en colaboración con la Universidad de Louisville (Estados Unidos), muestra cómo un corazón enfermo puede repararse a sí mismo. Los investigadores trataron a 16 pacientes que habían sufrido un infarto muy severo y lograron que su corazón se recuperara tras infundirle sus propias células madre cardiacas. Los resultados se publican en la revista médica «The Lancet» y «abren una nueva opción para los pacientes infartados con un mal pronóstico», asegura Anversa .
Un año después del tratamiento, el efecto continuaba. Es la primera vez que se demuestra el efecto de una terapia celular a tan largo plazo. Eso sí, con una ayuda técnica bastante potente, no solo con un «empujoncito» exterior. Para conseguirlo, los enfermos tuvieron que pasar primero por una biopsia de corazón y después por un cateterismo, una técnica no exenta de riesgo. En la biopsia se toma parte del tejido del corazón para después aislar y ampliar en el laboratorio las células madre reparadoras. Con el cateterismo posterior, se introduce un catéter por la arteria para llegar hasta el corazón y depositar las células.
Al producirse un ataque cardiaco, el infarto reduce la capacidad que tienen los ventrículos para bombear la sangre en un solo latido. Al disminuir el aporte sanguíneo, el tejido cardiaco se queda sin oxígeno y muere. Esas zonas necrosadas provocan un falllo cardiaco, porque la capacidad de bombeo se reduce.
-Cirugía y biopsia
Cuando el infarto es importante, a la mayoría de los pacientes se les ofrece una cirugía de «bypass», una suerte de puentes con vasos sanguíneos para sortear las zonas muertas y seguir nutriendo el resto del tejido. A los pacientes de este ensayo clínico también se les ofreció esta cirugía, momento que se aprovechó para tomar la biopsia. Una vez cultivadas, un millón de células madre cardiacas viajaron, de vuelta, hasta los corazones dañados con la única misión de tratar de regenerar los daños.
Durante un año, el equipo de investigadores siguió a los enfermos tratados y a otros siete pacientes con la misma dolencia que solo fueron sometidos a «bypass». Cuatro meses después de la terapia celular, el corazón de los pacientes mejoró su capacidad para bombear sangre y siguió mejorando un año después, fecha del último control. Las cicatrices típicas de las zonas muertas del infarto también habían mejorado. En cambio, los siete enfermos que solo fueron operados no notaron mejoría.
Cuando el infarto es importante, a la mayoría de los pacientes se les ofrece una cirugía de «bypass», una suerte de puentes con vasos sanguíneos para sortear las zonas muertas y seguir nutriendo el resto del tejido. A los pacientes de este ensayo clínico también se les ofreció esta cirugía, momento que se aprovechó para tomar la biopsia. Una vez cultivadas, un millón de células madre cardiacas viajaron, de vuelta, hasta los corazones dañados con la única misión de tratar de regenerar los daños.
Durante un año, el equipo de investigadores siguió a los enfermos tratados y a otros siete pacientes con la misma dolencia que solo fueron sometidos a «bypass». Cuatro meses después de la terapia celular, el corazón de los pacientes mejoró su capacidad para bombear sangre y siguió mejorando un año después, fecha del último control. Las cicatrices típicas de las zonas muertas del infarto también habían mejorado. En cambio, los siete enfermos que solo fueron operados no notaron mejoría.
-Terapia prometedora
Con tan pocos pacientes tratados, el ensayo clínico solo puede considerarse una estrategia prometedora que ha demostrado su seguridad. De momento no es una intervención sencilla para extenderla a la mayoría de los infartados, apunta Felipe Prosper, director del área de Terapia Celular de la Clínica de la Universidad de Navarra. La buena noticia es que es los resultados mejoraron con el tiempo y se mantuvieron durante más de un año. «Es la primera vez que se observan estos avances a largo plazo», afirma Prosper. Además de utilizar células cardiacas, otros investigadores han empleado células de la grasa y de la médula ósea para reparar corazones infartados.
Aunque los resultados se observaron con pruebas de imagen, tampoco se puede descartar que la mejoría se deba a efectos indirectos, como el que se despertaran células «durmientes» que ayudaran en la reparación. En un comentario editorial que acompaña a la investigación, Gerd Heusch, profesor de la Universidad de Essen rebosa optimismo: «Confiamos en que este estudio tenga el mismo potencial para transformar la terapia cardiaca que Escipión,(el único general romano capaz de derrotar a Aníbal) en su campaña contra Cartago».
Con tan pocos pacientes tratados, el ensayo clínico solo puede considerarse una estrategia prometedora que ha demostrado su seguridad. De momento no es una intervención sencilla para extenderla a la mayoría de los infartados, apunta Felipe Prosper, director del área de Terapia Celular de la Clínica de la Universidad de Navarra. La buena noticia es que es los resultados mejoraron con el tiempo y se mantuvieron durante más de un año. «Es la primera vez que se observan estos avances a largo plazo», afirma Prosper. Además de utilizar células cardiacas, otros investigadores han empleado células de la grasa y de la médula ósea para reparar corazones infartados.
Aunque los resultados se observaron con pruebas de imagen, tampoco se puede descartar que la mejoría se deba a efectos indirectos, como el que se despertaran células «durmientes» que ayudaran en la reparación. En un comentario editorial que acompaña a la investigación, Gerd Heusch, profesor de la Universidad de Essen rebosa optimismo: «Confiamos en que este estudio tenga el mismo potencial para transformar la terapia cardiaca que Escipión,(el único general romano capaz de derrotar a Aníbal) en su campaña contra Cartago».
**Publicado en "ABC"
El Real Betis lanza "Betis Lab", una innovación en salud

El Real Betis Balompié ha presentado un nuevo departamento de innovación en la entidad verdiblanca, BetisLab, una importante mejora en el área médica.
José Millán Acosta, director del área de salud del club, ha explicado que "Betis Lab no es más que una unidad de prevención de lesiones".
"Utilizaremos todos los elementos que se tienen en el Betis para analizarlos en un laboratorio y por sistemas de alarmas saber cuándo un jugador puede tener lesiones o problemas físicos, aunque las fortuitas no se pueden evitar lógicamente". Este centro médico seguirá línea de otros como el Benfica Lab o Milan Lab.
El objetivo del mismo "no se centra sólo en una categoría, se centra en todos los equipos de la cantera, que también entrarán en el Betis Lab". "Además tendremos pronósticos de déficit fisiológicos en cantera para que se puedan corregir a tiempo en jugadores jóvenes", ha explicado.
Asimismo, José Antonio Bosch ha definido Betis Lab como "nuestra I+D donde nosotros tenemos futuro y donde vamos a apostar fuerte porque no podemos competir con otros equipos que tiran de chequera, nosotros apostaremos por la cantera para ser competitivos en el futuro".
Por último, Tomás Calero, médico del club, también ha ofrecido su visión sobre este departamento: "La idea surge de que tropezamos en la misma piedra siempre, que el índice de lesiones no bajan de un año para otro. Tenemos la suerte de que el consejo de administración nos haya escuchado para poder abordar este problema. Valoraremos todo tipo de información y gracias a esas alarmas que antes se han mencionado se podrán prever posibles lesiones o problemas físicos con el consiguiente beneficio para el jugador y club. Cada 15 o 20 días sabremos qué jugadores tienen más alarmas y por tanto más posibilidades de tener lesión".
José Millán Acosta, director del área de salud del club, ha explicado que "Betis Lab no es más que una unidad de prevención de lesiones".
"Utilizaremos todos los elementos que se tienen en el Betis para analizarlos en un laboratorio y por sistemas de alarmas saber cuándo un jugador puede tener lesiones o problemas físicos, aunque las fortuitas no se pueden evitar lógicamente". Este centro médico seguirá línea de otros como el Benfica Lab o Milan Lab.
El objetivo del mismo "no se centra sólo en una categoría, se centra en todos los equipos de la cantera, que también entrarán en el Betis Lab". "Además tendremos pronósticos de déficit fisiológicos en cantera para que se puedan corregir a tiempo en jugadores jóvenes", ha explicado.
Asimismo, José Antonio Bosch ha definido Betis Lab como "nuestra I+D donde nosotros tenemos futuro y donde vamos a apostar fuerte porque no podemos competir con otros equipos que tiran de chequera, nosotros apostaremos por la cantera para ser competitivos en el futuro".
Por último, Tomás Calero, médico del club, también ha ofrecido su visión sobre este departamento: "La idea surge de que tropezamos en la misma piedra siempre, que el índice de lesiones no bajan de un año para otro. Tenemos la suerte de que el consejo de administración nos haya escuchado para poder abordar este problema. Valoraremos todo tipo de información y gracias a esas alarmas que antes se han mencionado se podrán prever posibles lesiones o problemas físicos con el consiguiente beneficio para el jugador y club. Cada 15 o 20 días sabremos qué jugadores tienen más alarmas y por tanto más posibilidades de tener lesión".
Subscribe to:
Posts (Atom)