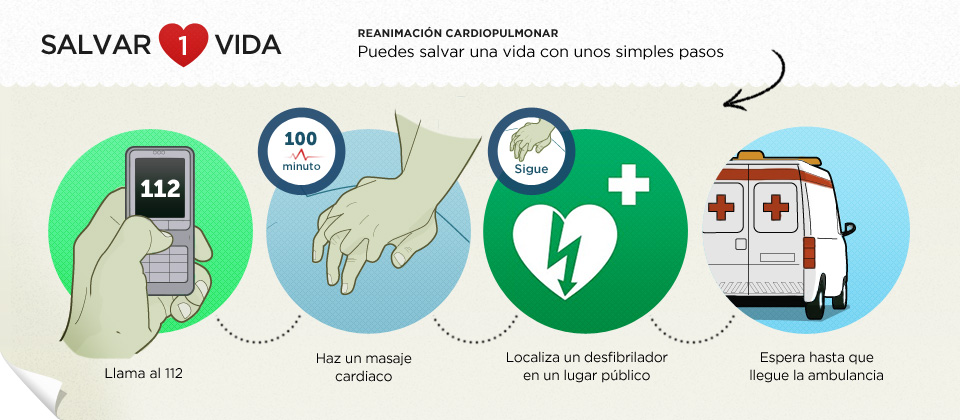
La dra. Nekane Murga, cardióloga en el Hospital de Basurto (Bilbao), ha puesto en marcha la iniciativa Salvar 1 Vida, un proyecto creativo que busca concienciar a la población sobre la necesidad de conocer las maniobras básicos de Reanimación Cardiopulmonar.
**En Twitter: #salvar1vida
Diario digital con noticias de actualidad relacionadas con el mundo de la salud. Novedades, encuestas, estudios, informes, entrevistas. Con un sencillo lenguaje dirigido a todo el mundo. Y algunos consejos turísticos para pasarlo bien
Traductor
06 July 2011
{kind=link}
El Hospital La Paz atendió a 57 niños de todo el mundo con Síndrome de Gorham
El Hospital Universitario La Paz de Madrid ha atendido a 57 niños de todo el mundo afectados por Síndrome de Gorham, estableciéndose como centro referente internacional para el tratamiento de dicha enfermedad rara de origen desconocido y con difícil diagnóstico. La Unidad de Anomalías Vasculares del Departamento de Cirugía Pediátrica de este hospital fue visitada por el consejero de Sanidad de la Comunidad de Madrid, Javier Fernández-Lasquetty. Se trata de uno de los pocos centros en el mundo que cuentan con amplia experiencia clínica al concentrar una importante serie de pacientes en estudio.
Así, La Paz se ha convertido en un punto de referencia no solo en España sino para otros países, ya que está atendiendo a pacientes procedentes de Francia, Italia, Bélgica, Finlandia, México, Chile, Colombia y Argelia. En algunos casos, el paciente es trasladado a la Comunidad de Madrid a través del Servicio Madrileño de Salud para confirmar el diagnóstico y realizar el tratamiento. En otros, los pacientes son tratados en su país de origen bajo la supervisión y asesoría de los especialistas de La Paz que, en alguna ocasión se desplazan hasta allí.
El síndrome de Gorham-Stout es una enfermedad rara que se cree que aparece por una proliferación de vasos linfáticos que produce la destrucción del hueso. La enfermedad, descrita ya en el siglo XIX, se produce en pacientes de todas las edades, desde niños de 1 mes hasta adultos de 75 años. Su diagnóstico puede ser difícil ya que es poco frecuente, no suelen aparecer hallazgos específicos con las técnicas de imagen convencionales como las radiografías y las tomografías y porque otras enfermedades como la Histiocitosis, la Osteolisis de otro origen y las metástasis, pueden presentar un aspecto similar.Reconocimiento tardíoA pesar de que esta enfermedad está bien descrita, no aparece con la frecuencia necesaria para que los médicos puedan reconocerla pronto y a veces pasan varios años hasta que se llega a su diagnóstico. Por ello, es poco frecuente que se conozca un caso de enfermedad de Gorham desde el primer síntoma. En la mayoría de los casos, la enfermedad no se reconoce hasta que se produce una fractura y se observa que el hueso comienza a desaparecer. Se cree que un traumatismo o un problema inmunológico inician la secuencia de acontecimientos posteriores que desencadenan la enfermedad.Para atender lo mejor posible a los pacientes que padecen enfermedades raras y dentro del estado actual de la ciencia médica, en el conjunto de los hospitales públicos de la Comunidad de Madrid hay 35 grandes grupos de diagnóstico de las diversas enfermedades raras. En cuanto a investigación, en la Comunidad de Madrid existen más de 30 grupos de investigación en el área de enfermedades genéticas, con más de 100 proyectos de investigación que integran el CIBER de Enfermedades Raras.
Así, La Paz se ha convertido en un punto de referencia no solo en España sino para otros países, ya que está atendiendo a pacientes procedentes de Francia, Italia, Bélgica, Finlandia, México, Chile, Colombia y Argelia. En algunos casos, el paciente es trasladado a la Comunidad de Madrid a través del Servicio Madrileño de Salud para confirmar el diagnóstico y realizar el tratamiento. En otros, los pacientes son tratados en su país de origen bajo la supervisión y asesoría de los especialistas de La Paz que, en alguna ocasión se desplazan hasta allí.
El síndrome de Gorham-Stout es una enfermedad rara que se cree que aparece por una proliferación de vasos linfáticos que produce la destrucción del hueso. La enfermedad, descrita ya en el siglo XIX, se produce en pacientes de todas las edades, desde niños de 1 mes hasta adultos de 75 años. Su diagnóstico puede ser difícil ya que es poco frecuente, no suelen aparecer hallazgos específicos con las técnicas de imagen convencionales como las radiografías y las tomografías y porque otras enfermedades como la Histiocitosis, la Osteolisis de otro origen y las metástasis, pueden presentar un aspecto similar.Reconocimiento tardíoA pesar de que esta enfermedad está bien descrita, no aparece con la frecuencia necesaria para que los médicos puedan reconocerla pronto y a veces pasan varios años hasta que se llega a su diagnóstico. Por ello, es poco frecuente que se conozca un caso de enfermedad de Gorham desde el primer síntoma. En la mayoría de los casos, la enfermedad no se reconoce hasta que se produce una fractura y se observa que el hueso comienza a desaparecer. Se cree que un traumatismo o un problema inmunológico inician la secuencia de acontecimientos posteriores que desencadenan la enfermedad.Para atender lo mejor posible a los pacientes que padecen enfermedades raras y dentro del estado actual de la ciencia médica, en el conjunto de los hospitales públicos de la Comunidad de Madrid hay 35 grandes grupos de diagnóstico de las diversas enfermedades raras. En cuanto a investigación, en la Comunidad de Madrid existen más de 30 grupos de investigación en el área de enfermedades genéticas, con más de 100 proyectos de investigación que integran el CIBER de Enfermedades Raras.
05 July 2011
Socioeconomic class and smoking linked to premature menopause
Women from the lowest social class are almost three times as likely to have premature ovarian failure (POF) as those from the highest social class, a researcher told the annual conference of the European Society of Human Reproduction and Embryology today (Wednesday). POF is not only associated with infertility but also with significantly increased morbidity and mortality, as well as a decreased quality of life equivalent to that of people with type 2 diabetes or rheumatoid arthritis, said Dr. Rumana Islam, from Imperial College, London, UK.
Previous studies of POF, defined as the onset of menopause before the age of 40, have assessed the small group of women who seek hospital care, and therefore there is little information about the risks and impacts of POF across a whole population, Dr. Islam explained. With her colleague Dr. Rufus Cartwright, she studied the records of nearly 5000 women who formed part of the 1958 Birth Cohort. "This included all the women born in Britain in a single week," explained Dr. Islam. "They have been followed up eight times, most recently at age 50, when they were asked about the date and cause of their menopause and also their quality of life."
Out of the 4968 study participants, 370, or 7.4%, had either spontaneous or medically induced POF. In addition to the influence of social class, there was a strong independent association with smoking. Quality of life was measured using the SF-36 health survey, which produces a profile of physical and psychological health and well-being in eight areas. Women with POF were more than twice as likely to report poor quality of life, and this effect was not eliminated by taking confounding factors such as smoking, obesity, and physical exercise into account. "There was also a profound impact on quality of life 10 years after POF, affecting vitality, physical function, mental health, and general health perceptions. However, social function was unaffected," said Dr. Islam.
POF is characterised by amenorrhea (the absence of periods), infertility, and sex steroid deficiency leading to menopausal symptoms in women aged under 40. Almost 20% of the women in the study who had undergone POF had done so as a result of early removal of the ovaries and/or hysterectomy, or as a consequence of chemotherapy. "While hysterectomy has become less common over the last decade, our findings reinforce the recommendation that it should be a last resort for menstrual disorders, and that oophorectomy should be avoided in younger women," said Dr. Islam.
The researchers say that they have shown, for the first time, in a large cohort, the huge unrecognised physical and psychological burden of women among the general population with POF. "This suggests an immediate need for primary care practitioners to screen for POF in women who present with amenorrhea before the age of 40," said Dr. Islam.
The average age at which women reach menopause is similar across different ethnic groups, and comparable findings are likely from other Western nations, the researchers say. "Socioeconomic influences on health are pervasive, but often hard to disentangle," said Dr. Islam. "Based on these data we can only speculate as to what they are, but the effect might be due to an unaccounted for environmental effect. Despite the availability of universal health care throughout these women’s lives, there might also be differences in access to health care or differences in health behaviours.
"However, our data provide a clear rationale for the management of POF symptoms by healthcare providers. We believe that women with POF can benefit from multidisciplinary specialist care, including support for their significant psychological and physical symptoms. Their long-term health needs should also be considered. Our study has shown POF has a major impact on the quality of life of a significant section of the population, and it needs addressing urgently," she concluded.
Previous studies of POF, defined as the onset of menopause before the age of 40, have assessed the small group of women who seek hospital care, and therefore there is little information about the risks and impacts of POF across a whole population, Dr. Islam explained. With her colleague Dr. Rufus Cartwright, she studied the records of nearly 5000 women who formed part of the 1958 Birth Cohort. "This included all the women born in Britain in a single week," explained Dr. Islam. "They have been followed up eight times, most recently at age 50, when they were asked about the date and cause of their menopause and also their quality of life."
Out of the 4968 study participants, 370, or 7.4%, had either spontaneous or medically induced POF. In addition to the influence of social class, there was a strong independent association with smoking. Quality of life was measured using the SF-36 health survey, which produces a profile of physical and psychological health and well-being in eight areas. Women with POF were more than twice as likely to report poor quality of life, and this effect was not eliminated by taking confounding factors such as smoking, obesity, and physical exercise into account. "There was also a profound impact on quality of life 10 years after POF, affecting vitality, physical function, mental health, and general health perceptions. However, social function was unaffected," said Dr. Islam.
POF is characterised by amenorrhea (the absence of periods), infertility, and sex steroid deficiency leading to menopausal symptoms in women aged under 40. Almost 20% of the women in the study who had undergone POF had done so as a result of early removal of the ovaries and/or hysterectomy, or as a consequence of chemotherapy. "While hysterectomy has become less common over the last decade, our findings reinforce the recommendation that it should be a last resort for menstrual disorders, and that oophorectomy should be avoided in younger women," said Dr. Islam.
The researchers say that they have shown, for the first time, in a large cohort, the huge unrecognised physical and psychological burden of women among the general population with POF. "This suggests an immediate need for primary care practitioners to screen for POF in women who present with amenorrhea before the age of 40," said Dr. Islam.
The average age at which women reach menopause is similar across different ethnic groups, and comparable findings are likely from other Western nations, the researchers say. "Socioeconomic influences on health are pervasive, but often hard to disentangle," said Dr. Islam. "Based on these data we can only speculate as to what they are, but the effect might be due to an unaccounted for environmental effect. Despite the availability of universal health care throughout these women’s lives, there might also be differences in access to health care or differences in health behaviours.
"However, our data provide a clear rationale for the management of POF symptoms by healthcare providers. We believe that women with POF can benefit from multidisciplinary specialist care, including support for their significant psychological and physical symptoms. Their long-term health needs should also be considered. Our study has shown POF has a major impact on the quality of life of a significant section of the population, and it needs addressing urgently," she concluded.
Giving up smoking as soon as pregnancy is confirmed averts the adverse birth outcomes associated with tobacco
Scientists have shown for the first time in a large population study that mothers’ stopping smoking around the time of getting pregnant can prevent the harmful effects of tobacco on their babies’ growth. Results from a study of over 50 000 pregnancies revealed that women who gave up smoking when their pregnancy was confirmed gave birth to babies with a similar birthweight to those born to mothers who had never smoked, Professor Nick Macklon, from the Department of Obstetrics and Gynaecology, University of Southampton, UK, told the annual conference of the European Society of Human Reproduction and Embryology today (Wednesday).
Low birthweight is the most common negative outcome of smoking during pregnancy, but foetuses exposed to maternal smoking are also at risk of premature birth and the associated problem of brain damage, as well as congenital abnormalities such as cleft lip. Mothers who smoke are encouraged to stop smoking when they become pregnant, but to date there was little evidence that giving up at this late stage could have a positive effect on birthweight.
Professor Macklon and colleagues decided to investigate this question by studying clinical, lifestyle, and socioeconomic data collected from pregnancies registered at the Southampton University Medical Centre between 2002 and 2010. They identified seven groups of women – non-smokers, those who had stopped more than a year prior to conceiving, those who had stopped less than a year prior to conceiving, smokers who stopped once the pregnancy was confirmed, and those who continued to smoke up to 10 a day, between 10 and 20 a day, and more than 20 a day. They proceeded to compare smoking behaviour in the mothers with perinatal outcomes in the children.
After correcting for gestational age, maternal age, BMI and socioeconomic class, all of which are known to affect birth outcomes, the researchers found that those babies whose mothers had stopped smoking in the periconceptional period – around the time of getting pregnant or as soon as the pregnancy was confirmed – had a significantly higher birthweight.
"Not only was birthweight much better in this group than it was in the groups where the mothers had continued to smoke, but we also found that the babies reached the same gestational age and head circumference as those born to women who had never smoked," said Professor Macklon. "While a recent study has shown that the rate of pre-term and small-for-gestational-age births can be reduced by stopping smoking before the 15th week of pregnancy, our research goes much further. We can now give couples hard evidence that making the effort to stop smoking in the periconceptional period will be beneficial for their baby."
Although there is now overwhelming evidence that maternal smoking during pregnancy is damaging to the foetus, some mothers continue to smoke because they like the idea of giving birth to a smaller baby. "It is important that people who believe that a smaller baby means an easier birth take into account the increased risks of complicated deliveries in smokers," said Professor Macklon, "as well as the risk of disease later in life which goes with low birthweight. Smoking during pregnancy is not just bad for the mother and baby, but for the adult it will grow into."
In addition to this, smoking can also make it more difficult for a woman to get pregnant and carry a baby to term. Because of their faster ovarian ageing, women smokers have higher rates of infertility than non-smokers and will undergo an earlier than normal menopause. They are also are more likely to have miscarriages.
"In future we would like to look at the impact of stopping smoking prior to fertility treatments, as we believe that this could bring about improvements to fertility outcomes," said Professor Macklon. "But for now we hope that our research will provide additional encouragement to mothers-to-be to give up cigarettes."
Low birthweight is the most common negative outcome of smoking during pregnancy, but foetuses exposed to maternal smoking are also at risk of premature birth and the associated problem of brain damage, as well as congenital abnormalities such as cleft lip. Mothers who smoke are encouraged to stop smoking when they become pregnant, but to date there was little evidence that giving up at this late stage could have a positive effect on birthweight.
Professor Macklon and colleagues decided to investigate this question by studying clinical, lifestyle, and socioeconomic data collected from pregnancies registered at the Southampton University Medical Centre between 2002 and 2010. They identified seven groups of women – non-smokers, those who had stopped more than a year prior to conceiving, those who had stopped less than a year prior to conceiving, smokers who stopped once the pregnancy was confirmed, and those who continued to smoke up to 10 a day, between 10 and 20 a day, and more than 20 a day. They proceeded to compare smoking behaviour in the mothers with perinatal outcomes in the children.
After correcting for gestational age, maternal age, BMI and socioeconomic class, all of which are known to affect birth outcomes, the researchers found that those babies whose mothers had stopped smoking in the periconceptional period – around the time of getting pregnant or as soon as the pregnancy was confirmed – had a significantly higher birthweight.
"Not only was birthweight much better in this group than it was in the groups where the mothers had continued to smoke, but we also found that the babies reached the same gestational age and head circumference as those born to women who had never smoked," said Professor Macklon. "While a recent study has shown that the rate of pre-term and small-for-gestational-age births can be reduced by stopping smoking before the 15th week of pregnancy, our research goes much further. We can now give couples hard evidence that making the effort to stop smoking in the periconceptional period will be beneficial for their baby."
Although there is now overwhelming evidence that maternal smoking during pregnancy is damaging to the foetus, some mothers continue to smoke because they like the idea of giving birth to a smaller baby. "It is important that people who believe that a smaller baby means an easier birth take into account the increased risks of complicated deliveries in smokers," said Professor Macklon, "as well as the risk of disease later in life which goes with low birthweight. Smoking during pregnancy is not just bad for the mother and baby, but for the adult it will grow into."
In addition to this, smoking can also make it more difficult for a woman to get pregnant and carry a baby to term. Because of their faster ovarian ageing, women smokers have higher rates of infertility than non-smokers and will undergo an earlier than normal menopause. They are also are more likely to have miscarriages.
"In future we would like to look at the impact of stopping smoking prior to fertility treatments, as we believe that this could bring about improvements to fertility outcomes," said Professor Macklon. "But for now we hope that our research will provide additional encouragement to mothers-to-be to give up cigarettes."
Enfermedades como la diabetes, la neumonía o la arterioesclerosis pueden agravarse por una higiene bucal defectuosa, según expertos
Una mala salud bucodental puede condicionar el desarrollo de enfermedades como la diabetes, determinadas alteraciones cardiovasculares y pulmonares, y provocar partos prematuros. Así lo aseguran especialistas de la Sociedad Española de Periodoncia y Osteointegración (SEPA) como David Herrera, Antonio Santos y Pedro Diz, que han analizado para Listerine las últimas evidencias científicas disponibles al respecto.Recientemente, las revistas ‘American Journal of Cardiology y Journal of Periodontology’ han publicado un documento de consenso sobre la relación entre las enfermedades cardiacas y las de las encías, en el que se recomienda a cardiólogos y odontólogos examinar tanto la boca del paciente como su historia cardiovascular.
Por su parte, la Academia Americana de Odontología ha establecido nuevas directrices que exigen asesoramiento sobre salud oral a las mujeres embarazadas. Los científicos también han encontrado datos que demuestran que las bacterias que crecen en la cavidad bucal pueden alcanzar los pulmones y provocar enfermedades como la neumonía, y que la enfermedad periodontal puede predisponer o agravar la diabetes. Según Herrera y Diz, estas asociaciones se producen fundamentalmente por el paso de las bacterias que causan la periodontitis desde la cavidad oral a la sangre (bacteriemia) y, por tanto, al resto del cuerpo.
Un fenómeno que viene condicionado por el grado de higiene oral, fundamentalmente por la acumulación de placa bacteriana y el nivel de gingivitis. Asimismo, según el doctor Diz, las bacteriemias también se han relacionado recientemente con el desarrollo de la arterioesclerosis, “aunque su significación clínica aún no se ha determinado definitivamente”.
Por su parte, la Academia Americana de Odontología ha establecido nuevas directrices que exigen asesoramiento sobre salud oral a las mujeres embarazadas. Los científicos también han encontrado datos que demuestran que las bacterias que crecen en la cavidad bucal pueden alcanzar los pulmones y provocar enfermedades como la neumonía, y que la enfermedad periodontal puede predisponer o agravar la diabetes. Según Herrera y Diz, estas asociaciones se producen fundamentalmente por el paso de las bacterias que causan la periodontitis desde la cavidad oral a la sangre (bacteriemia) y, por tanto, al resto del cuerpo.
Un fenómeno que viene condicionado por el grado de higiene oral, fundamentalmente por la acumulación de placa bacteriana y el nivel de gingivitis. Asimismo, según el doctor Diz, las bacteriemias también se han relacionado recientemente con el desarrollo de la arterioesclerosis, “aunque su significación clínica aún no se ha determinado definitivamente”.
Se presenta en el Congreso Europeo de ORL de Barcelona el implante coclear más pequeño y más sofisticado del mundo, ya disponible en España
El implante coclear de titanio más pequeño y ligero del mundo y también el más eficaz, fruto de un proceso intensivo de investigación y desarrollo, ya está disponible en España. El nuevo sistema de implantes auditivos MAESTRO 2010 contiene el implante más pequeño y ligero del mundo en encapsulado de titanio, lo que lo hace ideal para niños y también para adultos. Los implantes cocleares constituyen el primer caso de sustitución de un sentido mediante mecanismos externos, y un avance médico definitivo que está permitiendo reducir de forma considerable el número de personas sordas en el mundo. MAESTRO 2010 cuenta con un componente interno, que se inserta en la cóclea del oído medio, un 25 por ciento más fino que sus predecesores y diseñado para procedimientos quirúrgicos mínimamente invasivos.
El sistema se completa con las más finas y flexibles guías de electrodos y con un audio procesador externo, también el más pequeño y ligero del mundo, responsable de transformar los sonidos en señales eléctricas. MED-EL ha presentado MAESTRO 2010 y otros sistemas destinados a facilitar la audición en casos de pérdida auditiva, en un simposio celebrado durante el séptimo Congreso Europeo de Otorrinolaringología (ORL), que se celebra estos días en Barcelona con la asistencia de cerca de cuatro mil especialistas de todo el mundo.
La pérdida auditiva es una de las patologías más frecuentes en recién nacidos. En España se calcula que tres de cada mil recién nacidos presentan problemas de audición. De ellos, uno de cada tres tiene una pérdida profunda de audición, dos de cada tres una pérdida moderada, sin que se detecten diferencias por sexo. Más del 95 por ciento de los niños sordos nacen en el seno de familias oyentes. Desde que hace unos años se implantó el ‘screening’ obligatorio de capacidad auditiva en las maternidades españolas, se estima que cada año unos 800 bebés españoles reciben implantes cocleares, lo que, junto con la imprescindible rehabilitación posterior, les permite mantener un desarrollo y una curva de aprendizaje prácticamente similar a la de los niños oyentes.
Aproximadamente el mismo número de adultos sufrirá pérdida severa de la audición a lo largo de su vida, sobre todo a partir de los 50 años. En menores de 50 las causas de pérdida de audición suelen obedecer a otros factores, como accidentes, enfermedades infecciosas, cáncer o problemas auditivos previos que evolucionan.
-Los implantes cocleares en España
En España, la media de edad de los bebés que reciben un implante coclear es de quince meses; los implantes cocleares se pueden usar desde los primeros meses de vida. En nuestro país hay 165 implantados por millón de habitantes, de los que 95 son niños y 70 son adultos, es decir, más de 4.300 niños y casi 3.200 adultos españoles. En total 7.500 españoles llevan un implante coclear, el diez por ciento de los implantados europeos. Un implante coclear más doce años de rehabilitación tiene un coste de 71.000 a 95.000 euros. En el mismo período de tiempo, se pueden ahorrar entre 26.000 y 31.000 en costes de educación especial. Según datos del INE, en España existe alrededor de un millón de personas con discapacidad auditiva de distinto grado y tipo, de las cuales un diez por ciento tienen sordera profunda. El 90 por ciento son capaces de comunicarse mediante lenguaje oral.
**Publicado en "EL MEDICO INTERACTIVO"
El sistema se completa con las más finas y flexibles guías de electrodos y con un audio procesador externo, también el más pequeño y ligero del mundo, responsable de transformar los sonidos en señales eléctricas. MED-EL ha presentado MAESTRO 2010 y otros sistemas destinados a facilitar la audición en casos de pérdida auditiva, en un simposio celebrado durante el séptimo Congreso Europeo de Otorrinolaringología (ORL), que se celebra estos días en Barcelona con la asistencia de cerca de cuatro mil especialistas de todo el mundo.
La pérdida auditiva es una de las patologías más frecuentes en recién nacidos. En España se calcula que tres de cada mil recién nacidos presentan problemas de audición. De ellos, uno de cada tres tiene una pérdida profunda de audición, dos de cada tres una pérdida moderada, sin que se detecten diferencias por sexo. Más del 95 por ciento de los niños sordos nacen en el seno de familias oyentes. Desde que hace unos años se implantó el ‘screening’ obligatorio de capacidad auditiva en las maternidades españolas, se estima que cada año unos 800 bebés españoles reciben implantes cocleares, lo que, junto con la imprescindible rehabilitación posterior, les permite mantener un desarrollo y una curva de aprendizaje prácticamente similar a la de los niños oyentes.
Aproximadamente el mismo número de adultos sufrirá pérdida severa de la audición a lo largo de su vida, sobre todo a partir de los 50 años. En menores de 50 las causas de pérdida de audición suelen obedecer a otros factores, como accidentes, enfermedades infecciosas, cáncer o problemas auditivos previos que evolucionan.
-Los implantes cocleares en España
En España, la media de edad de los bebés que reciben un implante coclear es de quince meses; los implantes cocleares se pueden usar desde los primeros meses de vida. En nuestro país hay 165 implantados por millón de habitantes, de los que 95 son niños y 70 son adultos, es decir, más de 4.300 niños y casi 3.200 adultos españoles. En total 7.500 españoles llevan un implante coclear, el diez por ciento de los implantados europeos. Un implante coclear más doce años de rehabilitación tiene un coste de 71.000 a 95.000 euros. En el mismo período de tiempo, se pueden ahorrar entre 26.000 y 31.000 en costes de educación especial. Según datos del INE, en España existe alrededor de un millón de personas con discapacidad auditiva de distinto grado y tipo, de las cuales un diez por ciento tienen sordera profunda. El 90 por ciento son capaces de comunicarse mediante lenguaje oral.
**Publicado en "EL MEDICO INTERACTIVO"
Frozen embryo transfer leads to larger and heavier babies
Two studies from France and Denmark have shown that children born after frozen embryo transfer are larger and heavier. The risk for a baby to be too heavy for its gestational age at birth is increased 1.6 fold compared to IVF children from fresh embryo transfer and 1.5 fold compared to naturally conceived children, the 27th Annual Meeting of the European Society of Human Reproduction and Embryology will hear tomorrow (Wednesday).
In the first study, French scientists looked at neonatal outcome in terms of mode of delivery, gestational age, preterm birth rate (less than 37 weeks of gestation), mean child measurements, low birth weight (less than 2,500g) and perinatal mortality. When comparing the cryo singletons to the fresh cohort, the scientists showed that mean birth weight, mean height and head circumference were lower in the fresh population. The mean birth weight of the cryo babies was 102g higher compared to the fresh cohort. Low birth weight for children born to term (more than 37 weeks) was also significantly lower in fresh babies. Low birth weight to normal birth weight ratio was twice as high in the fresh population (3.6% compared to 1.8%).
“Frozen embryo transfer did not seem to adversely affect neonatal outcome,” says Dr. Sylvie Epelboin, from Bichat-Claude Bernard Hospital, Paris. “We are not sure why the cryo babies are heavier and larger, but we think it may have something to do with the hormonal hyperstimulation during the fresh cycles.”
The researchers found no significant difference between the two cohorts in terms of preterm birth rate and mode of delivery. However, the boys to girls ratio was 1.05 times higher in the cryo group as was the IVF/ICSI ratio (84% compared to 65%). The ratio of women who had given birth once to multiparous women was 1.6 times higher in the fresh cohort. The group analysed 16,002 singletons, 2,140 of these children were in the cryo group and 13,682 were from fresh embryo transfers.
-In a second study from Denmark Dr. Anja Pinborg and her group from the Rigshospital at Copenhagen University compared intrauterine parameters of 910 singletons born after frozen embryo transfer (FET) with 9,603 babies from fresh embryo transfer and 4,656 naturally conceived (NC) children. The rate of large-for-gestational age (LGA) babies was significantly different between the three groups with 16.9% for FET, 10.3% for fresh transfer and 11.4% for NC babies. The same applied to the rate of babies with birth weight of 4,500g or more (5.6%, 2.8% and 3.4% respectively).
“Cryopreservation of embryos can result in ‘Large Offspring Syndrome’, which may be explained by epigenetic changes in the very early embryonic stages caused by freezing and thawing procedures,” says Dr. Pinborg. “Future studies must look into the precise epigenetic changes causing LGA offspring in humans. In animal studies, there is evidence that abnormal gene expression of certain developmentally important genes may be responsible for the observed large offspring syndrome.”
The risk for a baby to be too heavy for the gestational age at birth is increased 1.6 fold compared to children from fresh embryo transfer and 1.5 fold compared to naturally conceived children. The group found a similar significant pattern for small-for-gestational age (SGA) children. Only 9.2% of FET singletons were SGA compared to 14.8% in fresh IVF and ICSI and 11.3% in NC children. > > “We think that because in FET cycles hormone supplementation mimics the natural cycle, compared to the superphysiologically high hormonal stimulation of women in fresh cycles, this ‘similar-to-natural-cycle concept’ may influence endometrial receptivity, early implantation and placental development in a positive way, leading to higher foetal growth and higher mean weight,” Dr. Pinborg will say.
Placenta previa (PP)* was seen in 0.9% of FET pregnancies compared to 1.5% of fresh IVF/ICSI and 0.3% of NC children. However, these figures were not significantly different and there was no association between PP and the risk of being SGA in any of the cohorts. “This lower risk in placenta previa in FET compared to the other groups may be explained with alterations in the endometrial contractility,” says Dr. Pinborg. “Ovarian stimulation and/or oocyte retrieval may induce alterations in the endometrial contractility leading to fewer implantation sites than in the unstimulated frozen cycles. The transcervical embryo replacement may also have some impact and hence lead to a higher placenta previa rate in FET compared to natural cycles.”> > Babies with a high birth weight may face an increased rate of delivery by Caesarean section and obstetric intervention causing complications for both mother and baby.
In the first study, French scientists looked at neonatal outcome in terms of mode of delivery, gestational age, preterm birth rate (less than 37 weeks of gestation), mean child measurements, low birth weight (less than 2,500g) and perinatal mortality. When comparing the cryo singletons to the fresh cohort, the scientists showed that mean birth weight, mean height and head circumference were lower in the fresh population. The mean birth weight of the cryo babies was 102g higher compared to the fresh cohort. Low birth weight for children born to term (more than 37 weeks) was also significantly lower in fresh babies. Low birth weight to normal birth weight ratio was twice as high in the fresh population (3.6% compared to 1.8%).
“Frozen embryo transfer did not seem to adversely affect neonatal outcome,” says Dr. Sylvie Epelboin, from Bichat-Claude Bernard Hospital, Paris. “We are not sure why the cryo babies are heavier and larger, but we think it may have something to do with the hormonal hyperstimulation during the fresh cycles.”
The researchers found no significant difference between the two cohorts in terms of preterm birth rate and mode of delivery. However, the boys to girls ratio was 1.05 times higher in the cryo group as was the IVF/ICSI ratio (84% compared to 65%). The ratio of women who had given birth once to multiparous women was 1.6 times higher in the fresh cohort. The group analysed 16,002 singletons, 2,140 of these children were in the cryo group and 13,682 were from fresh embryo transfers.
-In a second study from Denmark Dr. Anja Pinborg and her group from the Rigshospital at Copenhagen University compared intrauterine parameters of 910 singletons born after frozen embryo transfer (FET) with 9,603 babies from fresh embryo transfer and 4,656 naturally conceived (NC) children. The rate of large-for-gestational age (LGA) babies was significantly different between the three groups with 16.9% for FET, 10.3% for fresh transfer and 11.4% for NC babies. The same applied to the rate of babies with birth weight of 4,500g or more (5.6%, 2.8% and 3.4% respectively).
“Cryopreservation of embryos can result in ‘Large Offspring Syndrome’, which may be explained by epigenetic changes in the very early embryonic stages caused by freezing and thawing procedures,” says Dr. Pinborg. “Future studies must look into the precise epigenetic changes causing LGA offspring in humans. In animal studies, there is evidence that abnormal gene expression of certain developmentally important genes may be responsible for the observed large offspring syndrome.”
The risk for a baby to be too heavy for the gestational age at birth is increased 1.6 fold compared to children from fresh embryo transfer and 1.5 fold compared to naturally conceived children. The group found a similar significant pattern for small-for-gestational age (SGA) children. Only 9.2% of FET singletons were SGA compared to 14.8% in fresh IVF and ICSI and 11.3% in NC children. > > “We think that because in FET cycles hormone supplementation mimics the natural cycle, compared to the superphysiologically high hormonal stimulation of women in fresh cycles, this ‘similar-to-natural-cycle concept’ may influence endometrial receptivity, early implantation and placental development in a positive way, leading to higher foetal growth and higher mean weight,” Dr. Pinborg will say.
Placenta previa (PP)* was seen in 0.9% of FET pregnancies compared to 1.5% of fresh IVF/ICSI and 0.3% of NC children. However, these figures were not significantly different and there was no association between PP and the risk of being SGA in any of the cohorts. “This lower risk in placenta previa in FET compared to the other groups may be explained with alterations in the endometrial contractility,” says Dr. Pinborg. “Ovarian stimulation and/or oocyte retrieval may induce alterations in the endometrial contractility leading to fewer implantation sites than in the unstimulated frozen cycles. The transcervical embryo replacement may also have some impact and hence lead to a higher placenta previa rate in FET compared to natural cycles.”> > Babies with a high birth weight may face an increased rate of delivery by Caesarean section and obstetric intervention causing complications for both mother and baby.
Subscribe to:
Posts (Atom)
CONTACTO · Aviso Legal · Política de Privacidad · Política de Cookies
Copyright © Noticia de Salud